Case Study
Semaglutide Lead Generation With Meta Instant Forms
This case study explains how IMR generated high-volume semaglutide program leads using Meta native Instant Forms with segmentation, compliance-forward creative, and qualification-first form design.
Meta lead forms can produce volume fast. However, volume alone does not build trust. Therefore, this case study focuses on what we can verify, how we measured it, and what we deliberately did not claim.
We ran Meta Lead Ads using native Instant Forms. Additionally, we separated campaigns to control cost, intent, and messaging. Because this clinic offered a nationwide shipping model as well as local care, we structured acquisition to match both realities instead of forcing one generic funnel.
We report results from the most recent 30-day reporting window inside Meta Ads Manager. We also explain attribution limits, quality controls, and the exact steps we followed so readers can reuse the framework responsibly.
Table Of Contents
Case Study Snapshot
- Industry: Health & wellness clinic offering a semaglutide weight loss program.
- Market/Location: Hybrid model: local clinic plus nationwide shipping program.
- Starting point (baseline): The client wanted predictable lead flow without relying on a website-only funnel.
- Primary goal: Generate qualified leads for the semaglutide program at a sustainable cost per lead while maintaining compliance-forward messaging.
- Constraints: We did not have closed-won revenue or CRM close-rate reporting available during this window, so we focused on lead acquisition metrics and validation controls.
- Channels used: Meta (Facebook/Instagram) Lead Ads with native Instant Forms.
- Measurement stack: Meta Ads Manager lead reporting and lead form delivery logs; additionally, we reviewed form design, qualification logic, and campaign segmentation to validate intent controls.
- Outcome summary (no invented numbers): We generated 271 leads across three semaglutide-related lead campaigns inside the 30-day window, with reported costs per lead of $4.86, $4.99, and $9.52, respectively.
Because this case study uses Meta native forms, you will see a different measurement approach than a typical landing-page funnel. Therefore, we prioritize clarity around what the platform reports and what you should validate next.
The Challenge
Direct Answer: We needed to generate semaglutide program leads at scale while keeping messaging compliant, intent high, and reporting honest even without close-rate data.
Health and wellness acquisition brings two problems at the same time. First, advertisers must keep copy careful, because policies restrict certain approaches and claims. Next, clinics must protect lead quality, because low-friction forms can attract low-intent submissions if you do not add smart filters.
Additionally, the clinic operated a hybrid model. That model increased opportunity, because it expanded the serviceable market. However, it also increased complexity, because local intent and nationwide intent behave differently in creative, offer framing, and follow-up urgency.
Finally, we did not have closed-won metrics available during this reporting window. Therefore, we chose a truth-first structure: we would prove what we observed, we would document what we did, and we would label any inference clearly as an inference.
What We Could Measure Reliably In 30 Days
- Lead volume by campaign inside Meta Ads Manager.
- Cost per lead by campaign inside Meta Ads Manager.
- Form completion behavior signals (for example, higher-intent questions and contact info completion).
What We Could Not Measure Reliably In 30 Days
- Revenue, ROAS, or profit impact, because we did not receive closed-won reporting.
- Appointment show rate, because we did not receive scheduling disposition data.
- Long-term retention or LTV, because we evaluated a short time window.
Strategy (What We Did And Why)
We built the strategy around one principle: reduce friction, then add intentional friction. That sounds contradictory. However, it works because the right friction increases intent while still keeping the process easy for qualified prospects.
1) Campaign Segmentation To Control Intent
We separated acquisition into distinct campaigns rather than blending all audiences into one. Therefore, each campaign could carry its own creative angle, its own qualification posture, and its own optimization path. Additionally, segmentation made cost and volume easier to interpret, because each campaign represented one structured hypothesis instead of a mixed bag.
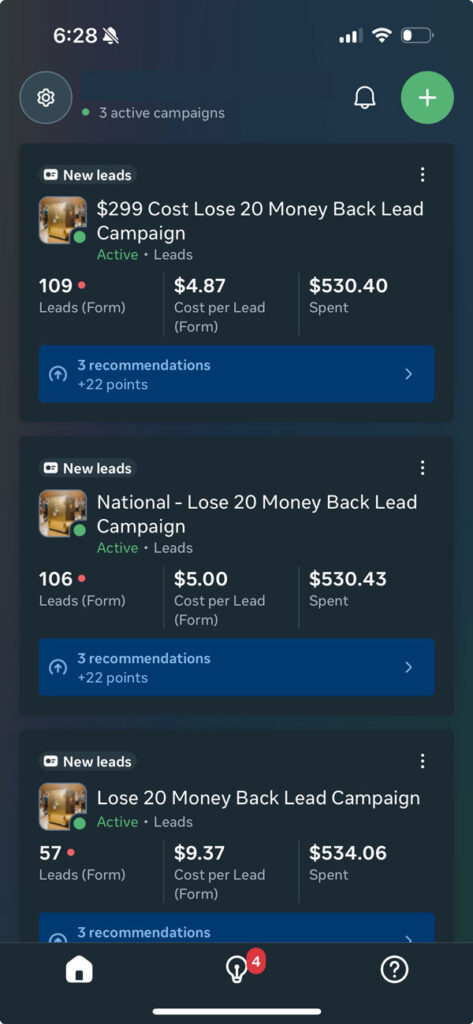
During this window, the clinic ran three semaglutide lead campaigns that produced the following Meta-reported outcomes:
- Campaign A: 109 leads at $4.86 cost per lead.
- Campaign B: 106 leads at $4.99 cost per lead.
- Campaign C: 56 leads at $9.52 cost per lead.
Because we did not receive additional metadata about which campaign mapped to local versus nationwide, we did not assign those labels here. Instead, we focus on the system that produced stable acquisition across multiple campaign lanes.
2) Creative Built For Clarity, Not Shock
We used videos and images in every campaign. Additionally, we crafted copy carefully so it stayed direct while still respecting platform policy and consumer trust. We leaned into a Hormozi-style hook pattern for clarity and speed, because short, specific headline structures reduce confusion and help the algorithm learn faster.
However, we did not use hype. Instead, we focused on:
- Clear program framing (what it is, who it serves, and what happens next).
- Clear expectation setting (what the lead form collects and how the clinic follows up).
- Clear separation of education versus claims (what we explain versus what we promise).
3) Instant Forms For Speed, Then Qualification For Intent
Meta Lead Ads with Instant Forms reduce drop-off because the platform pre-fills contact fields for many users. Therefore, conversion rates often increase compared to website-only flows. However, if you remove all friction, you often attract low-intent leads. So, we added a single qualification question inside the form to reduce noise while protecting volume.
We used one qualification question on purpose. First, one question keeps friction low. Next, one question still filters out a meaningful segment of casual clickers. Additionally, one question makes follow-up easier because the team can route leads by that answer.
4) Compliance-Forward Messaging As A Growth Strategy
In health and wellness, compliance is not a legal afterthought. Instead, compliance becomes a performance lever, because compliant messaging builds trust and reduces disapprovals. Therefore, we built copy that avoided personal-attribute targeting language and avoided unrealistic claims.
We also kept the offer simple and measurable: “submit a form to get program details and next-step instructions.” That approach supports user expectations and reduces confusion. Consequently, the clinic can follow up consistently, which then improves downstream outcomes even when we cannot report those outcomes yet.
Implementation (Step-by-Step)
Because this case study must support repeatable execution, we document the implementation as a practical checklist. Additionally, we include decision rules so teams can adapt the process to their own constraints.
- Define the lead as a measurable event.
We defined a lead as a completed Meta Instant Form submission that included the required contact fields and the single qualification question. Therefore, our reporting stayed consistent across campaigns.
- Separate campaigns by intent lane.
We built separate campaigns so each lane carried a clear hypothesis. For example, one lane can prioritize broad discovery, while another lane can prioritize higher-intent framing. Then, we compared CPL and volume across lanes rather than guessing inside one blended campaign.
- Create “hook-first” primary text and headlines.
We used concise, direct, Hormozi-style headline logic to communicate value quickly. Additionally, we aligned the hook with the form promise, so users did not feel bait-and-switch during submission.
- Build creative sets with controlled variation.
We deployed videos and images per campaign. Then, we varied one element at a time—hook angle, visual framing, or value explanation—so optimization stayed interpretable.
- Configure Instant Forms for high-intent collection.
We used a single qualification question to add intentional friction. Additionally, we kept the rest of the form simple so completion stayed high.
- Set follow-up expectations inside the form.
We communicated what happens next and how the clinic contacts the lead. Therefore, users understood the process and the clinic reduced confusion-driven drop-off.
- Align compliance and clarity before scaling spend.
We reviewed messaging for compliance-forward language and avoided unrealistic promises. Then, we scaled only after the creative and the form worked together cleanly.
- Monitor cost and volume daily, then adjust weekly.
We checked performance daily to catch sudden shifts. However, we made structural changes weekly so the algorithm could learn rather than reset constantly.
- Validate lead logs and remove anomalies.
We reviewed lead delivery logs and watched for obvious anomalies (for example, repeated entries). Therefore, we preserved data quality even without CRM disposition reporting.
- Document learnings for the next 30 days.
We recorded which hooks and creatives produced stable CPL. Then, we prepared a follow-up plan that focuses on deeper qualification and closed-loop tracking.
Decision Rules We Used While Implementing
- If CPL stays low but lead quality concerns rise, then increase qualification friction gradually by adding one additional question or tightening answer options.
- If CPL rises sharply after edits, then revert the last change and allow the learning phase to stabilize before trying a different lever.
- If one campaign dominates volume, then keep it stable while testing variations in a separate lane, so you protect baseline performance.
- If policy risk increases, then simplify claims and remove personal-attribute phrasing, because compliance protects both delivery and trust.
Measurement & Validation
Measurement becomes the center of a trustworthy case study. Therefore, we separate observed facts, methods, and inferences clearly.
Observed Facts (Client/Platform Reported)
- Channel: Meta Lead Ads using native Instant Forms.
- Timeframe: Most recent 30-day reporting window.
- Campaign structure: Separate campaigns with video and image creative.
- Qualification: One qualification question inside the form.
- Meta-reported outcomes for the semaglutide program:
- 109 leads at $4.86 cost per lead.
- 106 leads at $4.99 cost per lead.
- 56 leads at $9.52 cost per lead.
Methods Used (IMR Process)
- We structured campaigns to keep intent lanes separate and measurable.
- We wrote hook-first copy while prioritizing clarity and compliance-forward language.
- We used Instant Forms for reduced friction, then we used one qualification question for intent control.
- We validated lead delivery logs and reviewed campaign-level stability across the 30-day window.
Inferences / Hypotheses (Clearly Labeled)
- Inference: Segmentation likely improved interpretability of CPL by reducing cross-contamination between intents.
- Inference: The qualification question likely reduced some low-intent submissions, because qualification friction generally filters casual clicks.
- Inference: Compliance-forward creative likely improved delivery stability, because policy-safe messaging reduces disapprovals and reduces volatility.
Attribution Limits (Why We Stay Truth-First)
Meta Instant Forms live inside the platform, so they reduce website dependence. However, they also shift what you can track easily. Additionally, multi-touch attribution varies by platform and by reporting model. Therefore, we do not claim revenue impact without closed-loop validation.
Data Quality Controls We Recommend Next
- Connect lead delivery to a CRM pipeline stage so you can measure contacted, qualified, booked, and closed outcomes.
- Use consistent naming conventions across campaigns so you can reconcile Meta reporting with downstream systems.
- Implement call tracking or scheduling event tracking if the clinic routes leads into calls or bookings.
- Record the qualification answer and tie it to sales outcomes, because that link lets you optimize for quality rather than volume alone.
What We Can Prove
- We can prove lead volume and cost per lead as reported by Meta Ads Manager during the 30-day window.
- We can prove the acquisition method: Meta Lead Ads with native Instant Forms and one qualification question.
- We can prove the campaign approach: separate campaigns with tailored creative and careful copy.
What We Cannot Claim
- We cannot claim ROAS, revenue, profit, or lifetime value from this window, because we did not receive closed-won reporting.
- We cannot claim medical outcomes or guaranteed weight loss, because outcomes vary and compliance requires substantiation and careful claims.
- We cannot claim that every lead converted into an appointment or purchase without CRM disposition data.
Results (Truth-First)
Results matter. However, trustworthy results require context. Therefore, we present results exactly as provided and avoid invented assumptions.
30-Day Lead Volume And Cost Per Lead (Meta Reported)
- Campaign A: 109 leads at $4.86 CPL.
- Campaign B: 106 leads at $4.99 CPL.
- Campaign C: 56 leads at $9.52 CPL.
Across these three campaigns, the clinic generated 271 Meta-reported leads in the 30-day window. Additionally, the clinic maintained low reported CPLs while keeping a qualification step in the form.
Operational Wins (Direction-Only, No Invented Metrics)
- Cleaner analysis: Campaign segmentation simplified decisions because each lane represented a defined hypothesis.
- Faster learning: Hook-first creative clarified the offer quickly, so the system could learn who engaged.
- Intent control: The single qualification question added friction strategically, therefore the clinic could reduce some low-intent submissions while still keeping forms easy.
- Compliance posture: Careful copy reduced policy risk, so the clinic could run consistently rather than constantly rebuilding ads after disruptions.
What These Results Mean (And What They Do Not Mean)
These results mean the clinic achieved efficient lead acquisition in Meta’s native ecosystem during the reporting window. However, these results do not automatically translate into revenue without follow-up systems and closed-loop measurement. Therefore, the next phase should connect lead acquisition to qualification and conversion outcomes.
Lessons & Reusable Framework
When you run health and wellness acquisition, you need a system you can repeat safely. Therefore, we summarize the framework as a checklist plus decision rules.
Reusable Checklist: Meta Instant Form Lead Engine For Regulated Categories
- Start with compliance-forward messaging, then validate clarity before you scale.
- Use Instant Forms for speed, then add one high-signal qualification question for intent.
- Segment campaigns by intent lane so you can interpret results cleanly.
- Test creative with controlled variation so you learn fast without chaos.
- Write hooks that match the form promise, because alignment reduces confusion.
- State next-step expectations in the form so follow-up feels predictable.
- Review lead logs regularly, then remove obvious anomalies quickly.
- Plan phase two before you launch, because closed-loop tracking takes time to wire up.
If/Then Decision Rules
- If CPL stays low but quality concerns rise, then tighten the qualification question first before you change targeting.
- If CPL rises after a creative refresh, then roll back the refresh and test a smaller change next.
- If campaigns fluctuate daily, then reduce edits and allow learning, because constant resets create instability.
- If policy risk appears, then simplify language and remove personal-attribute phrasing immediately.
- If the clinic expands nationally, then separate local and nationwide intent lanes clearly, because follow-up and eligibility differ.
What We Would Improve Next (Process-First)
Next, we would connect leads to outcome stages. Then, we would optimize for qualified leads instead of raw leads. Additionally, we would test a second qualification lever only after we confirm the first lever improves downstream conversion.
We would also document the exact dates of the reporting window directly inside the case study once the clinic confirms them. Therefore, the page stays verifiable and audit-friendly.
FAQs
Does this case study prove revenue from semaglutide leads?
Direct Answer: No—this case study proves lead volume and Meta-reported cost per lead, because we did not receive closed-won revenue or close-rate reporting.
Revenue requires closed-loop measurement through a CRM or scheduling system. Therefore, we keep claims limited to what we can verify inside the reporting window.
Why did IMR use Meta Instant Forms instead of a website landing page?
Direct Answer: We used Instant Forms because they reduce friction and often increase completion rates, then we added a qualification question to protect intent.
Instant Forms also simplify the user path. However, they require stronger follow-up discipline, so we recommend closed-loop tracking in phase two.
How did you keep lead quality from collapsing with low-friction forms?
Direct Answer: We used one qualification question and segmented campaigns by intent lane, so we could filter noise and interpret performance clearly.
Additionally, we aligned hooks with the form promise, so users self-selected more accurately before submitting.
Are the CPL numbers guaranteed for every clinic or market?
Direct Answer: No—CPL varies by market, offer clarity, compliance posture, creative quality, and follow-up systems.
Therefore, we treat this as a documented 30-day window outcome, not a universal promise.
What compliance constraints influenced creative and copy?
Direct Answer: We prioritized compliance-forward language and avoided unrealistic outcomes and personal-attribute phrasing to reduce policy risk and protect trust.
Because health advertising requires careful substantiation and responsible messaging, we kept copy clear, conservative, and expectation-led.
What would make this case study stronger in the next update?
Direct Answer: Closed-loop tracking from lead to contacted, qualified, booked, and closed outcomes would strengthen the proof and improve optimization.
Then, we could report qualified lead rate and cost per qualified lead with clear definitions and dates.
How many campaigns did you run for this clinic?
Direct Answer: We ran multiple separate campaigns with tailored creative, and we report three semaglutide lead campaigns with their lead counts and CPLs for this window.
Segmentation improved clarity. Therefore, we could compare lanes rather than guessing inside a blended structure.
What do you mean by “truth-first” results?
Direct Answer: We report only verified platform metrics and clearly label any inference, so the case study stays compliant, credible, and audit-friendly.
That approach also builds stronger long-term authority, because readers can trust the difference between facts, methods, and hypotheses.